Responsable : Guillaume Lefèvre
Workpackage : WP3
Background
Eosinophils are multifunctional leukocytes (white blood cells) involved in the pathogenesis of numerous inflammatory disorders, such as parasitic helminth, bacterial, and viral infections, tissue injury and fibrosis, anti-tumoral immunity, and allergic diseases. Eosinophils differentiate in the bone marrow and are recruited from peripheral blood to inflammatory tissues in response to chemoattractant signals. Then, when recruited in the tissues, eosinophils will exert their functions in response to diverse local stimuli. Likely depending on the eosinophil subtype and the tissue microenvironment, eosinophils may exert either toxic/pro-inflammatory functions or regulatory/repair roles (1,2). This is supported by recent studies that associate certain eosinophil phenotypic characteristics with either damaging pro-inflammatory or beneficial regulatory functions in mice (3–6). However, the identification of different eosinophil phenotypes or subtypes, and the comparison of these subtypes among different eosinophilic disorders are still needed in humans (3,4,7–12). This lack of knowledge must be addressed because depending on the type of eosinophilic disorder, some subtypes of eosinophils may have a role in controlling local inflammation and contributing to repair of damaged tissues rather than a harming role in pathogenesis (13). For instance, the presence of multiple types of eosinophils could explain the suspected different endotypes of ‘allergic diseases’ in which the role of eosinophils and/or type-2 (T2) inflammation is inconstant, and eosinophil targeting strategies disappointing (14,15).
Therefore, blood eosinophils, which have been understudied so far, may benefit from better characterization. According to the literature and our data, we hypothesize that after bone marrow terminal differentiation, blood eosinophils become already 'pre-activated' or “primed” before entering tissues, and the priming depends on the inflammatory context and the type and/or severity of the disease. To test our hypothesis and to carry this translational research we rely on our multidisciplinary group of physicians and scientists who has expertise in a variety of eosinophilic diseases, such as asthma, atopic dermatitis, chronic rhinitis, and rare conditions called ‘hypereosinophilic syndromes’ (HES) in which eosinophils are highly overproduced and have striking damaging functions in tissues.
It is our hope that the improved characterization of phenotypic and functional signatures of blood eosinophils will enhance the understanding of eosinophilic disorders and lead to new precision medicine strategies to better treat our patients.
Our research projects.
Our team conducts translational research projects in multiple eosinophilic disorders with two primary objectives:
- To establish associations between the phenotypic signature, the molecular profiles, and the functions of eosinophils in T2-mediated diseases, with the goal of assessing the role and specificity of eosinophil subsets and defining eosinophilic endotypes in these inflammatory disorders.
- To assess the underlying mechanisms in rare HES subtypes and to develop therapeutic strategies with appropriate available targeted therapies.
The research group.
University hospital physicians
- Dr. Frédéric DEZOTEUX, MD, PhD, Dermatology
- Dr. Guillaume LEFEVRE, MD, PhD (HDR), Immunology
- Pr. Geoffrey MORTUAIRE, MD, PhD (HDR), Otolaryngology
- Pr. Delphine STAUMONT-SALLE, MD, PhD (HDR), Dermatology
Senior scientist
- Dr. Stéphane ESNAULT, PhD (also affiliated with Dr. Jarjour Lab, University-Hospital of Wisconsin, USA)
Engineers
- Emilie ANGLO, MSc
- Arnaud DENDOOVEN, MSc
PhD students
- Matthieu GROH, MD
- Emeline DELAUNAY, MSc
Our research group belongs to the CEREO, national reference center for hypereosinophilic syndromes
Collaborations :
- • Pr. Cécile CHENIVESSE, MD, PhD, Pulmonology, Department of Allergy and Pulmonology, University of Lille-Hospital, Institut Pasteur de Lille, Centre d’Infection et d’Immunité de Lille, INSERM U1019, CNRS UMR9017, Univ. Lille, CRISALIS Network
- • Dr. Nicolas DUPLOYEZ, MD, PhD, Department of Hematology, University of Lille-Hospital, Inserm U1277, Canther (Cancer Heterogeneity, Plasticity and Resistance to Therapies)
- • Pr. Olivier HERMINE, MD, PhD, Head of the Department of Hematology, Necker Hospital, and University of Paris Descartes - Molecular mechanisms of hematological disorders and therapeutic implications, Inserm Unit U1163/ CNRS ERL 8254, Imagine Institute, and national reference center for systemic mastocytosis – CEREMAST, Paris

Detailed projects
Eosinophils in the DRESS syndrome, the DRESSEo project
Drug Reaction with Eosinophilia and Systemic Symptoms (DRESS) is a severe, life-threatening drug hypersensitivity associated with severe organ damage. Circulating blood eosinophil (Eos) count during drug hypersensitivity does not appear to reflect the involvement of Eos in the occurrence of skin or organs damages. Therefore, we may ask whether the phenotype rather than the number of Eos would better predict the impact of the Eos on skin or organ damages. In fact, no studies had been conducted to identify phenotypic signatures of Eos in the field of drug hypersensitivity.
Through a prospective multi-center approach, our group aims to assess the phenotypic profile of Eos in the skin and other organs through the development of an original and automated method for the detection of degranulation in tissues and the phenotypic signature of blood Eos in case of drug hypersensitivity group of patients.
Our approach will help us to distinguish the functional duality of circulating (Figure 1) and tissue Eos (in skin and other organs, Figure 2). The mechanisms underlying the differential activation of Eos according to compartments (blood/skin/organs) are currently clarified to better target the therapeutic management of patients. Our group coordinates a European multicenter clinical trial which will evaluate efficacy and tolerance of benralizumab, an eosinophil-depleting monoclonal antibody. First inclusions are planned for semester-1 of 2024.
Our group coordinates a European multicenter clinical trial which will evaluate efficacy and tolerance of benralizumab, an eosinophil-depleting monoclonal antibody. First inclusions are planned for semester-1 of 2024.
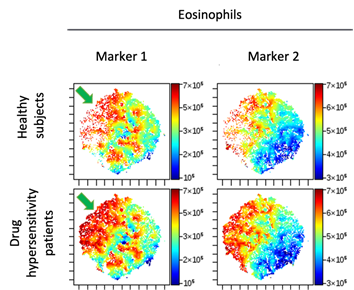
Figure 1. Graphical distribution of surface markers by t-SNE approach. After quantification of surface markers by flow cytometry, Eos are graphically grouped by their immunophenotypic similarities. Surface markers expression is visualized by color intensity, ranging from dark blue (lowest expression) to dark red (highest expression). Phenotypic heterogeneity of circulating Eos with the presence of a subpopulation overexpressing CD69 (marker 1, green arrow) or HLA-DR (marker 2).
.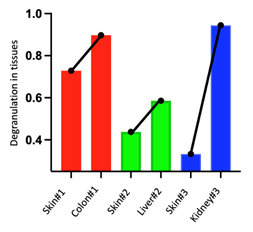
Figure 2. Comparison of Eos degranulation (16) in skin and organs from three patients with DRESS. The degranulation level is higher in the organs than in the skin during DRESS. These data highlight variations from patients to patients and from skin to organ in the same patient. This underlines the interest of considering Eos phenotypes and functions rather than just the number of blood Eos to predict the level of Eos activity/degranulation in tissues.
Eosinophils in atopic dermatitis, the ADEO project
As in other type-2 (T2) immune response diseases, atopic dermatitis (AD) may be accompanied by increase blood eosinophil (Eos) count. A role for Eos in the pathophysiology of this disease is therefore suspected but not yet elucidated. The arrival of new treatments targeting either the T2 immune response in AD (dupilumab, anti IL4/13; tralokinumab anti-IL13) or cytokines involved in the activation and chemotaxis of Eos, justifies the need to identify the phenotypic profiles of Eos along with the assessment of the impact of such treatments in patients. As a result, establishing that a certain treatment is more efficient for a specific Eos phenotype will ultimately allow the clinician to predict what treatment to give to a patient presenting a certain Eos phenotype.
Through a prospective multi-center approach, our group aims to assess the phenotypic profile of circulating Eos by flow cytometry and FlowSom analysis in AD patients who presented a moderate or severe form of AD and healthy subjects.
Preliminary data. While AD patients have a mean count of blood Eos closely identical to healthy controls (<0,5G/L), the mean fluorescence intensity (MFI) expression of surface markers is modified as visualized by cluster analysis using the FlowSOM algorithm compared with healthy controls (Figure 3). This data emphasizes that the phenotype of Eos is more important than the Eos number. Our team aims to explore the mechanisms that support the different Eos phenotypes and the functions of Eos with such phenotypes in AD. We will then clarify the exact role of Eos in AD and the impact on therapeutic management.
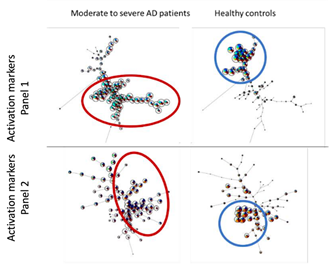
Figure 3. Cluster analysis of AD patients (red) and healthy subjects (blue) using the FlowSOM algorithm in Cytobank software. Each circle represents a sub-population of Eos defined by a similar MFI on the analyzed surface markers. The closer the circles, the closer the Eos profiles.
Eosinophils in severe chronic rhinosinusitis and severe asthma: the BIOPOSE and the PLEIAD projects
Eosinophils (Eos) are often considered as the pathologic landmark of chronic rhinosinusitis with nasal polyps (CRSwNP) in the field of T2 diseases. Many publications on CRSwNP emphasize the pivotal role of Eos in mucosal remodeling by their innate action via the degranulation of cytotoxic proteins. Eos recruitment from the bloodstream to the nasal mucosa requires the intricate action between the nasal epithelium, epithelial cell-activated type-2 (T2) innate lymphoid cells and adaptive immune cells secreting alarmins, cytokines and specific chemokines (17).
We proved in previous studies that the biological profile of patients with CRswNP is predictive of the therapeutic response to corticosteroids and surgery (18). We also showed that allergy was not pivotal to defining the inflammatory signature of these patients whereas comorbid asthma was associated with more severe CRSwNP and higher risk of symptomatic relapse (19,20).
New biologic agents capable of blocking T2 cytokines have been developed in the field of eosinophil-associated diseases, shifting the paradigm of treatment for patients with CRSwNP. A French registry about biologics in CRSwNP (BIOPOSE: BIOlogics in severe nasal POlyposis SurvEy - NCT05228041) is promoted by our group to define the best clinical and biological criteria to choose this promising therapeutic option. Comprehensive analysis of Eos phenotypes will be associated to delineate specific activation and priming profile.
Our preliminary data suggest that the proteome of nasal secretions is different between patients with or without asthma. In addition, we are conducting some unsupervised proteomics and transcriptomics approaches comparing nasal polyps in patients with or without asthma to understand the inflammatory mechanisms involved in nasal polyps depending on asthma status. Besides, we are conducting a comparative study of eosinophil phenotypes between severe asthma patients (w/o CRSwNP), severe chronic CRSwNP (w/o severe asthma) and healthy controls by global gene expression analyses of peripheral eosinophils (PLEIAD study, NCT NCT04187976).
These studies will help define Eos phenotypes in chronic rhinosinusitis and asthma. In future experiments, we hope to identify the cause(s) leading to the development of these phenotypes, the potential functions of these phenotypes in tissues, and consequently what is the best treatment(s) to tamper the damaging effects of the Eos in patients.
Eosinophils and mast cells interaction in systemic mastocytosis, the MASTEO study
Bidirectional interactions between eosinophils and mast cells (MCs) have been reported in various allergic diseases (21). Bone marrow (BM) eosinophilia is usual in systemic mastocytosis (SM), but its meaning has never been studied.
We collected BM biopsies from indolent SM (ISM) patients, smouldering SM (SSM), advanced SM (Adv-SM), and healthy controls. Using an automatized unsupervised analysis of whole slides (Figure 4), we observed that eosinophil peroxidase (EPX) staining (reflecting intact eosinophils plus eosinophil degranulation) was higher in non-advanced SM compared to controls and to Adv-SM. In addition, we observed positive correlations between serum tryptase levels with percentages of eosinophil in BM aspirations, eosinophils count in BM biopsies, EPX staining and eosinophil degranulation. Eosinophil count in BM biopsies also correlated with MC counts and c-KIT staining surface. We observed that eosinophil infiltrates and large areas of EPX deposition (i.e., eosinophil degranulation) were present within or around MC infiltrates. We also demonstrated that BM MCs expressed receptors for interleukin-5 (Figure 5), -9, -3 and for chemokines PGD2, eotaxins and TARC, which may contribute to interactions with eosinophils. Furthermore, next-generation sequencing of sorted blood eosinophils suggests that eosinophil proliferation is not clonal, and blood eosinophils display multiple phenotypes.
In summary, our data suggest that eosinophils and MCs may interact in tissues, and that eosinophils could contribute to tryptase release by MCs, and to MCs activation related symptoms. Thanks to these data that are the subject for a manuscript in preparation, we are now building a clinical trial evaluating anti-IL-5 antibody in non-advanced SM.
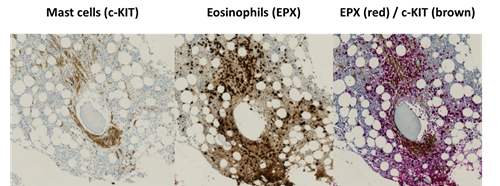
Figure 4. Dense eosinophil infiltrates with large degranulation area within a focal paratrabecular MCs infiltrates in bone marrow biopsy (indolent systemic mastocytosis).
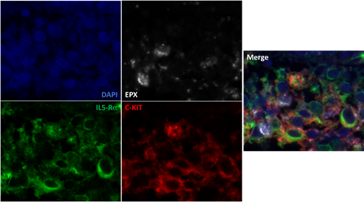
Figure 5. Assessment of IL-5Ra expression by MCs in ISM by immunofluorescence and confocal microscopy. MCs (EPX-c negative KIT positive cells, red) express surface IL5-Rα (green)
Eosinophils in hypereosinophilic syndromes (HES)
Neoplastic hypereosinophilia (HE) or hypereosinophilic syndrome (HES) are due to a clonal proliferation of eosinophils, with or without involvement of other lineages. The most frequent genetic cause is a gene fusion leading to the constitutive activation of tyrosine kinases (TK) such as PDGFRA, PDGFRB or FGFR, but somatic mutations of JAK1, STAT5B or JAK2 were recently reported in neoplastic eosinophils (22–24). We aimed to study the JAK-STAT pathway more extensively in normal eosinophils and in unexplained neoplastic hypereosinophilia or hypereosinophilic syndrome. We observed some new mutations in the JAK-STAT pathway and the benefit of JAK inhibitors in these patients (manuscript submitted).
Secondly, lymphocytic variant HES is due to a clonal proliferation of abnormal T cells with an aberrant CD3-CD4+ phenotype, which produce IL-5 that is responsible for the development of a secondary hypereosinophilia (25). Better characterization of abnormal T cells (26) led to evaluating the anti-CCR4 therapeutic antibody, mogamulizumab in this condition at high-risk of transformation in angioimmunoblastic T cell lymphoma, a poor prognosis lymphoma (27). A manuscript is submitted about the demonstration of the role of anti-CCR4 on T cells, in vitro, and on the benefit of mogamulizumab in severe CD3-CD4+ lymphocytic HES patients. In addition, using whole exome sequencing, we aim at understanding the underlying molecular mechanisms involved in this indolent clonal T cell lymphoproliferative disorders with reactive HE/HES.
These works on HES are conducted within the scope of the CEREO, national reference center for hypereosinophilic syndromes, and is supported by the COHESion network, COHEsion being a national cohort of more than 750 HE/HES patients included since May 2019. This cohort is coordinated by our group (NCT04018118) and a European expansion is planned in 2024.
References
1. Jacobsen EA, Taranova AG, Lee NA, Lee JJ. Eosinophils: Singularly destructive effector cells or purveyors of immunoregulation? J Allergy Clin Immunol 2007;119:1313–1320.
2. Rosenberg HF, Dyer KD, Foster PS. Eosinophils: changing perspectives in health and disease. Nat Rev Immunol 2013;13:9–22.
3. Mesnil C, Raulier S, Paulissen G, Xiao X, Birrell MA, Pirottin D et al. Lung-resident eosinophils represent a distinct regulatory eosinophil subset. J Clin Invest 2016;126:3279–3295.
4. Rothenberg ME. A hidden residential cell in the lung. 2016. doi:10.1172/JCI89768
5. Chen Z, Andreev D, Oeser K, Krljanac B, Hueber A, Kleyer A et al. Th2 and eosinophil responses suppress inflammatory arthritis. Nat Commun 2016;7:11596.
6. Andreev D, Liu M, Kachler K, Llerins Perez M, Kirchner P, Kölle J et al. Regulatory eosinophils induce the resolution of experimental arthritis and appear in remission state of human rheumatoid arthritis. Ann Rheum Dis 2021;80:451–468.
7. Johansson MW. Activation states of blood eosinophils in asthma. Clin Exp Allergy 2014;44:482–498.
8. Johansson MW. Eosinophil Activation Status in Separate Compartments and Association with Asthma. Front Med 2017;4:75.
9. Metcalfe DD, Pawankar R, Ackerman SJ, Akin C, Clayton F, Falcone FH et al. Biomarkers of the involvement of mast cells, basophils and eosinophils in asthma and allergic diseases. World Allergy Organ J 2016;9:7.
10. Lingblom C, Andersson J, Andersson K, Wennerås C. Regulatory Eosinophils Suppress T Cells Partly through Galectin-10. J Immunol 2017;198:4672–4681.
11. Johnsson M, Bove M, Bergquist H, Olsson M, Fornwall S, Hassel K et al. Distinctive blood eosinophilic phenotypes and cytokine patterns in eosinophilic esophagitis, inflammatory bowel disease and airway allergy. J Innate Immun 2011;3:594–604.
12. Matucci A, Nencini F, Maggiore G, Chiccoli F, Accinno M, Vivarelli E et al. High proportion of inflammatory CD62Llow eosinophils in blood and nasal polyps of severe asthma patients. Clin Exp Allergy J Br Soc Allergy Clin Immunol 2023;53:78–87.
13. Lee JJ, Jacobsen EA, McGarry MP, Schleimer RP, Lee NA. Eosinophils in health and disease: the LIAR hypothesis. Clin Exp Allergy J Br Soc Allergy Clin Immunol 2010;40:563–575.
14. Kang EG, Narayana PK, Pouliquen IJ, Lopez MC, Ferreira‐Cornwell MC, Getsy JA. Efficacy and safety of mepolizumab administered subcutaneously for moderate to severe atopic dermatitis. Allergy 2020;75:950–953.
15. Dellon ES, Peterson KA, Mitlyng BL, Iuga A, Bookhout CE, Cortright LM et al. Mepolizumab for treatment of adolescents and adults with eosinophilic oesophagitis: a multicentre, randomised, double-blind, placebo-controlled clinical trial. Gut 2023;72:1828–1837.
16. Dezoteux F, Bongiovanni A, Tardivel M, Dendooven A, Gibier J-B, Mortuaire G et al. Automatic quantification method of eosinophilic degranulation in tissues: Application for the study of eosinophilic disorders. Clin Exp Allergy J Br Soc Allergy Clin Immunol Published Online First: 18 April 2023. doi:10.1111/cea.14323
17. Vanderhaegen T, Gengler I, Dendooven A, Chenivesse C, Lefèvre G, Mortuaire G. Eosinophils in the Field of Nasal Polyposis: Towards a Better Understanding of Biologic Therapies. Clin Rev Allergy Immunol Published Online First: 2021. doi:10.1007/s12016-021-08844-7
18. Mortuaire G, Gengler I, Carpentier C, Szymanski C, Chenivesse C, Lefevre G. T helper 2 inflammatory markers are associated with recurrence in chronic rhinosinusitis with nasal polyps after endoscopic sinus surgery. Rhinology 2020;58:444–450.
19. Mortuaire G, Gengler I, Balden M, Capron M, Lefèvre G. Impact of allergy on phenotypic and endotypic profiles of nasal polyposis. Eur Ann Otorhinolaryngol Head Neck Dis 2018;135:159–162.
20. Mortuaire G, Gengler I, Vandenhende-Szymanski C, Delbeke M, Gatault S, Chevalier D et al. Immune profile modulation of blood and mucosal eosinophils in nasal polyposis with concomitant asthma. Ann Allergy Asthma Immunol Off Publ Am Coll Allergy Asthma Immunol 2015;114:299-307.e2.
21. Galdiero MR, Varricchi G, Seaf M, Marone G, Levi-Schaffer F, Marone G. Bidirectional Mast Cell–Eosinophil Interactions in Inflammatory Disorders and Cancer. Front Med 2017;4. doi:10.3389/fmed.2017.00103
22. Shomali W, Damnernsawad A, Theparee T, Sampson D, Morrow Q, Yang F et al. A novel activating JAK1 mutation in chronic eosinophilic leukemia. Blood Adv 2021;5:3581–3586.
23. Cross NCP, Hoade Y, Tapper WJ, Carreno-Tarragona G, Fanelli T, Jawhar M et al. Recurrent activating STAT5B N642H mutation in myeloid neoplasms with eosinophilia. Leukemia 2019;33:415–425.
24. Patel AB, Franzini A, Leroy E, Kim SJ, Pomicter AD, Genet L et al. JAK2 ex13InDel drives oncogenic transformation and is associated with chronic eosinophilic leukemia and polycythemia vera. Blood 2019;134:2388–2398.
25. Roufosse F. Hypereosinophilic syndrome variants: diagnostic and therapeutic considerations. Haematologica 2009;94:1188–1193.
26. Ledoult E, Groh M, Kahn J-E, Trauet J, Bouaziz J-D, Caristan A et al. Assessment of T-cell polarization on the basis of surface marker expression: Diagnosis and potential therapeutic implications in lymphocytic variant hypereosinophilic syndrome. J Allergy Clin Immunol Pract 2020;8:1110-1114.e2.
27. Lefèvre G, Copin M-C, Roumier C, Aubert H, Avenel-Audran M, Grardel N et al. CD3-CD4+ lymphoid variant of hypereosinophilic syndrome: nodal and extranodal histopathological and immunophenotypic features of a peripheral indolent clonal T-cell lymphoproliferative disorder. Haematologica 2015;100:1086–1095.